Joints
Where two (or more) bones join, or articulate.
The amount of movement possible is dependent on the type of joint.
- Abduction is movement away from the midline
- Adduction is a move towards towards the midline.
- Flexion is a decrease in the joint angle
- Extension is an increase in the joint angle.
Synovial joints
Synovial - enclosed in a joint capsule and are more mobile.
e.g. knee, shoulder, hip.
The amount of movement at each joint will vary between people. This may be limited by age, level of activity or disease.
It is important that we don’t apply pressure (force) to these joints directly to stop movement.
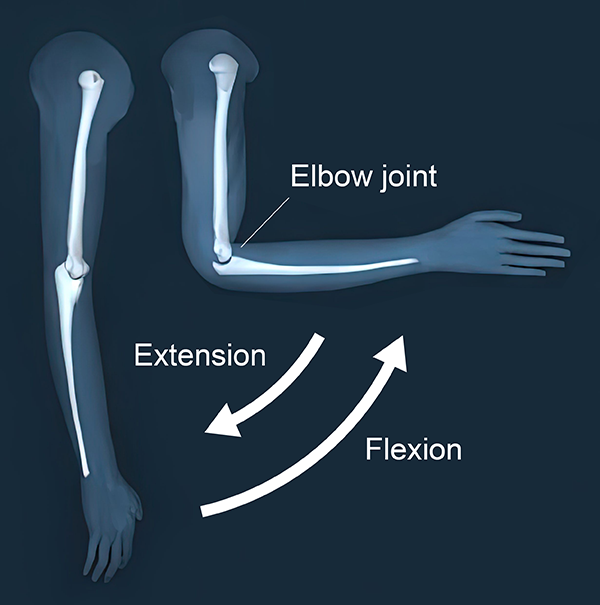
Hinge joints
One example of a hinge joint is the elbow. The movements at hinge joints are flexion and extension.
Hinge joints are moveable joints (e.g. knee, elbow) and it is important that we don’t apply pressure (force) to these joints directly to stop movement.
Remember we can flex (bend) at the knee and elbow with quite a larger range of movement. You cannot extend (straighten) with as much range of movement.
However, people with postural distortion, cerebral palsy, physical disabilities etc. may not have the same ranges of movement.
Ball and Socket Joints
One example of a ball and socket joint is the shoulder. The movements at ball and socket joints include flexion and extension, abduction and adduction, and medial and lateral rotation.
Ball and socket joints are moveable joints (e.g. shoulder and hip) and it is important that we don’t apply pressure (force) to these joints directly to stop movement. Ball and socket joints are able to move in three directions (axis), which we may want to limit during clinical holding.
However, people with postural distortion, cerebral palsy, physical disabilities etc. may not have the same ranges of movement.
Fibrous & Cartilaginous
Fibrous
Joined by connective tissue with usually no movement allowed e.g. skull, teeth.
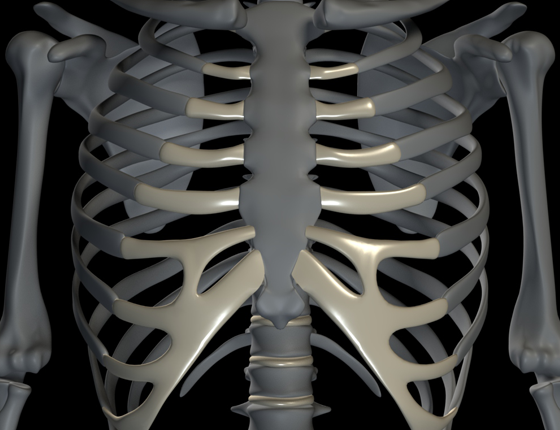
Cartilaginous
Joined by hyaline cartilage or fibrocartilage, minimal movement e.g. ribs with sternum.
Warning
Safety reasons - remember you must not apply pressure to the head or neck. Do not restrict breathing by placing pressure on the chest, for example ‘bear hugging’
In babies, the bones and joints of the skull (and other joints such as the shoulder) are not fully formed - particular care should be taken.
Immobilising joint movement within a clinical hold
Bones, muscle and tendons form levers which allow for movement in the human body.
The joint is the pivot (or axis) for the lever system and the muscles which cross the joint apply a force to move the resistance (bone).
We can see an example of this at the elbow joint.
The bicep applies a force to the radius to move the resistance.
Joints as Levers
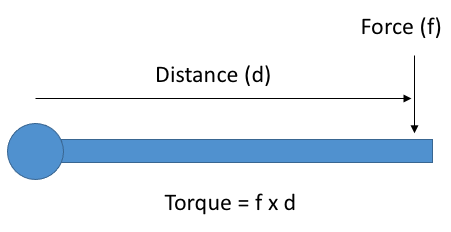
The movement of the bone around the axis is a rotational movement.
The force of this rotation (torque) can be calculated by multiplying the applied force (resistance or force) by the distance from the axis.
This is important for clinical holding. If we increase the distance between our hold and the joint, we can reduce the amount of force required.
For example, if we want to prevent a child from bending their arm we could hold their arm close to the elbow.
Or we could hold their arm at the wrist. By increasing the distance from the joint (pivot) we can use less force to achieve the same torque.
Activity
Hold your hand out palm down and apply pressure (force) at the upper arm, lower arm and top of the hand. Which position requires the least force to stop movement.
Considering these principles with procedures which may require clinical holds such as taking blood

Taking blood from the back of the hand - 1/7
In this position we need to look at clinical holding techniques to immobilise the child’s arms and legs.
We do not want the child to be able to move the arm that is having blood taken.
We also need to minimise movement from their other arm and their legs to prevent the child from hurting the nurse or parent/guardian.
It is important to have the child in a position where they can be distracted from the procedure.
Remember to allow some movement in the child’s limbs which do not need to be immobilised.
Taking blood from the back of the hand - 2/7
The child’s arm that isn’t having blood taken is placed behind the parent/guardian/nurse.
The parent/guardian/nurse controls movement at the shoulder and at the child’s thighs.
Notice the child’s lower legs are still free to move.
Taking blood from the back of the hand - 3/7
The hand here stops the child moving at the shoulder.
There is no gripping pressure from the parent/guardian/nurse.

Taking blood from the back of the hand - 4/7
The hand here stops the child moving at the hips/thigh.
There is no gripping pressure from the parent/guardian/nurse.

Taking blood from the back of the hand - 5/7
Remember the shoulder and hip are both ball and socket joints. They can move in three ways (flexion and extension, abduction and adduction, and rotation) which we need to control.
Taking blood from the back of the hand - 6/7
A nurse or parent/guardian will be required to immobilise the child’s hand to enable blood to be taken.
They need to control movement at the elbow and hand, whilst also constricting the blood vessels to allow easy identification of the vein in the hand.

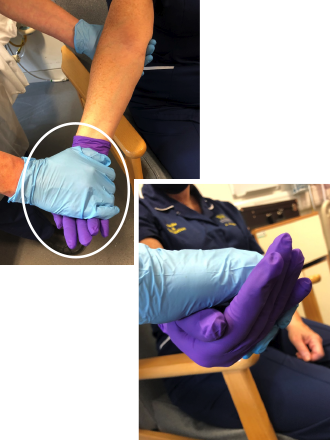
Taking blood from the back of the hand - 7/7
Holding the child’s fingers flexes the wrist to allow for blood to be taken.
Notice how the nurse ensures the thumb of the child is also within their control (to prevent the child from being able to squeeze their hand).
Holding near the wrist prevents movement at the elbow. It also constricts the blood vessels.
This can be done holding under the arm or below.
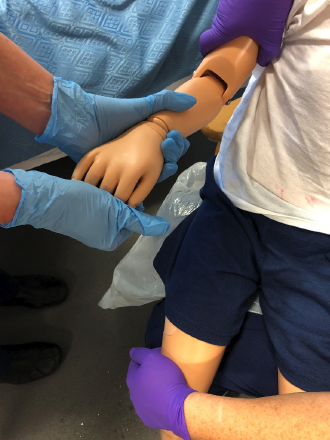
Taking blood from the antecubital fossa (child) - 1/3
The child can be positioned in the same way.
The child’s arm that isn’t having blood taken is placed behind the parent/guardian/nurse.
The parent/guardian/nurse controls movement at the shoulder and the child’s thighs.
Notice the child’s lower legs are still free to move.

Taking blood from the antecubital fossa (child) - 2/3
The child’s arm is supported under the elbow.
The principles of joints and leverage are applied here in that the nurse is able to prevent the child from flexing their elbow to escape the hold.
Remembering how the joint works as a lever, if we apply resistance near the hand (far from the joint/pivot) it makes it more difficult for the child to flex their elbow.
Taking blood from the antecubital fossa (child) - 3/3
Again the thumb is kept close to the palm of the hand, preventing the child from squeezing the nurse’s hand.
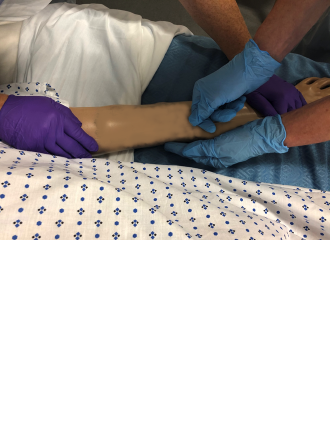
Taking blood from the antecubital fossa (adult in bed) - 1/2
In this an example an older patient is in bed and requires blood to be taken from the antecubital fossa.
One nurse controls movement at the shoulder, by placing their hand over the patient’s shoulder and onto their upper arm, and at the elbow by placing their hand at the patient’s wrist.
A second nurse is then able to take the blood sample/insert the cannula.
This hold works well to prevent flexion (bending) at the elbow as we apply force as far from the joint as possible.
By increasing the distance between the force and the joint we can reduce the amount force applied to the patient’s arm.

Taking blood from the antecubital fossa (adult in bed) - 2/2
Again the thumb is kept close to the palm of the hand, preventing the patient from squeezing the nurse’s hand.
Applying slight pressure on the hand helps to immobilise the arm by controlling elbow movement. Remember, having a large distance from the application of force and the joint means less force is required.
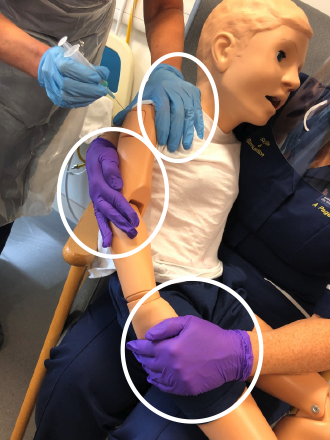
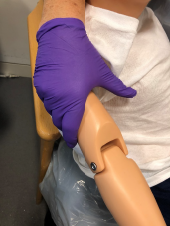
Intramuscular Injection (child) - 1/1
Here the upper arm needs to be exposed and controlled to allow for the clinical procedure, which in this case is a intramuscular injection.
The parent/guardian/nurse can keep the child’s arm close to their body by applying pressure above the elbow.
Movement at the elbow is controlled by holding the child’s hand. This position also allows the parent/guardian/nurse to control the child’s leg movement.
The nurse giving the injection can stabilise the shoulder with their spare hand, preventing the child leaning forward to get away if needed.
Key learning
- Movement occurs around joints
- When immobilising a limb it is important to use the least amount of force/pressure (strength). This can only be achieved by maximising the distance between the joint and the area where you are applying pressure
- There are very few instances where a grip is needed to immobilise the patients’ movement. By applying pressure in the correct area and in the correct direction the amount of strength required from the nurse/parent or guardian is reduced
- Under no circumstances must any pressure be applied to a joint
- Remember to allow some movement in the child’s limbs which do not need to be immobilised and their torso (chest) should never be constricted
Now that you have thought about how the body moves, think about the principles in relation to clinical holding. To do this now look at the Clinical holds Tool and then the Framework for Clinical Holding
Developed by Dr Chris Hartley, Dr Andrea Page & Alison Warren